
Q&A: Digital Breast Tomosynthesis
Reading Time: 4 minutes read
Ron Muscosky, Worldwide Product Line Manager, HCIS, Carestream
Digital breast tomosynthesis (DBT) is becoming increasingly popular in healthcare, but there are still many uncertainties surrounding it. Below are common questions healthcare organizations are asking about DBT and it is my goal to provide as thorough and accurate of answers as possible to demonstrate this technology’s value.
1. What is DBT and how does it differ from/compare to traditional mammograms?
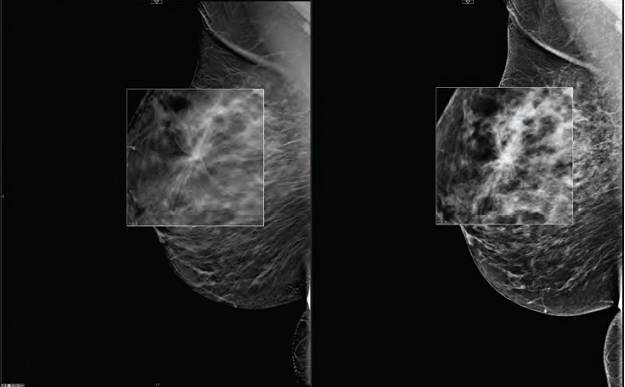
DBT is a mammography procedure that uses low dose X-rays to create a three-dimensional image of the breast. Also referred to as ‘3D mammography’, the tomosynthesis scanner partially rotates around the breast and takes about 10 to 15 images from many different angles. As with traditional mammograms, the breast is compressed during the exam. The radiologist can then view the breast tissue in narrow slices, similarly to CT scan images.
2. What benefits does DBT provide to physicians and patients?
With two-dimensional mammography, overlapping tissue can mask suspicious areas. Since thin layers of breast tissue are viewed with DBT, the overlap is removed and abnormalities are much easier to recognize. Studies have shown improved tissue identification, improved tumor visualization, and a lower recall rate for additional testing. Because of this, digital breast tomosynthesis has the potential to improve on the accuracy of mammography.
3. What are the challenges health facilities face when implementing DBT?
Financial: Cost is a challenge due to the lack of reimbursement. As patients become more aware of the benefits that DBT can bring, they’re asking for it. Even with the lack of reimbursement, many facilities are adding DBT to prevent a loss of patients to other facilities offering this technology, and/or to provide better patient care.
Technical: Technical challenges include the size and format of DBT data. DBT images can be very large, several times the size of conventional mammograms, so the transfer and storage of this data can be challenging. Additionally, some acquisition device vendors have been generating data in a proprietary format (due to the lack of a DICOM standard format in the past), and in some cases still storing data in a proprietary format. This presents challenges for healthcare facilities looking to standardize their data or use a mixture of vendor products.
Product: As healthcare facilities add DBT to their breast imaging procedures, many are finding that their existing storage and viewing solutions do not yet support this technology. This presents the facilities with the challenge of how they are going to store and view this data.
Workflow: DBT creates more data than a a conventional mammogram, increasing the time to read a case. Just like when digital mammography was first introduced, users are experiencing a learning curve with reading the images with the use of workstations and the tools they provide. In addition, some workstation vendors have very limited, if any, tools to optimize the reading of DBT exams, which magnifies the challenge.
4. How do providers overcome these challenges?
Financial: Some facilities are absorbing the costs by marketing the value of DBT and bringing in more patients. Others are charging the customer an extra fee to help offset the costs.
Technical: The data size challenge is overcome by careful planning of the network infrastructure and storage requirements. Acquisition device manufacturers are recommending a 1Gbps network to accommodate the image transfers, so facilities are either planning for this when building new or upgrading their existing infrastructure. We have found that in addition to adequate network bandwidth, the use of lossless compression and intelligent routing/pre-fetching of data are extremely important to efficiently move such large amounts of data around transparently to the user. This is especially true when reading is performed across multiple facilities and/or remotely.
Regarding the data format, DICOM now supports a new SOP Class that specifies how such data can be transmitted in a standardized format for interoperability between various vendors’ equipment. Most acquisition device vendors have adopted this standard, but existing proprietary data, and in some cases newly acquired data, still remain in proprietary formats. To address this issue, some acquisition device vendors are offering a service where the proprietary data can be converted to DICOM standardized data. This needs to be planned for ahead of any implementation of DICOM compliant equipment, since the conversion process can take some time to complete.
Product: Facilities that add DBT and find their existing solutions don’t support this technology are faced with either waiting for their existing solution to support this technology or purchasing another product that will provide such capabilities. Due to the importance of DBT, many facilities are choosing to replace or adjunct their existing solution with a product that supports this technology.
Workflow: We believe the learning curve radiologists are experiencing with the DBT technology will decrease over time, just as it did with digital mammography when it was first available.
The tools provided by an equipment vendor can also significantly decrease the time to read a DBT exam. It is important that a facility chooses a product with the appropriate tools to optimize their workflow. This includes not only the basic tools that automatically scale and position both 2D and 3D images, but also advanced tools that can help localize pathology and allow one to quickly navigate both current and prior studies. With conventional mammography, digital breast tomosynthesis, synthetic 2D mammography, and other mammography procedures being generated (e.g. breast US, breast MRI, etc.), workstations with hanging protocols that can support and display all of these in an efficient manner become extremely important as well.
5. What are the key points you hope attendees will take away from your panel discussion at SIIM?
Although there are a number of challenges with implementing DBT, solutions exist for each challenge and that will only improve in time as the technology matures. It is also important for attendees to plan their environment and product selections, knowing what challenges have been faced by others and how they have been resolved.
Editor’s Note: Ron will be participating in a panel session on “Problems and Solutions in Breast Tomosynthesis” during SIIM 2014. The session will be held on Thursday, May 15 from 12-1 pm in Exhibit Hall B – Innovation Theater.

